

Abstract
Introduction:
In limited-stage diffuse large B-cell lymphoma (DLBCL), a continued risk of relapse has been reported (Stephens et al. J Clin Oncol 2016). Another report highlighted that initial limited-stage DLBCL, a favorable International Prognostic Index and extranodal involvement seemed to be risk factors for late relapse (LR; Larouche et al. J Clin Oncol 2010). However, even if a subgroup of patients (pts) with LR shows distinct clinical characteristics, the underlying biology is largely unknown.
Methods:
Nineteen consecutive pts who developed LR were identified among 337 pts with de novo DLBCL of Ann Arbor stage I/II who were treated with CHOP (cyclophosphamide, doxorubicin, vincristine and prednisolone), with/without rituximab, between 1997 and 2012. LR was defined as the first relapse of B-cell lymphoma (BCL; including indolent BCL) occurring more than 5 years after a primary diagnosis. The 19 pts underwent clinical, pathological (cell of origin according to the Hans algorithm) and genetic analyses.
Genomic DNA (gDNA) was extracted from formalin-fixed, paraffin-embedded sections of tumor specimens at primary diagnosis and relapse, and from bone marrow (BM) specimens without tumor invasion as controls. Genomic DNA samples from paired primary and relapsed tumors were analyzed using BIOMED-2 multiplex PCR for immunoglobulin heavy chain (IGH) rearrangements (Invivoscribe Technologies, San Diego, CA, USA) to determine whether the paired tumors shared the same clonal IGH rearrangements.
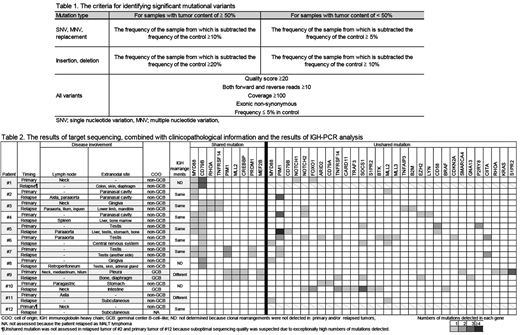
Target sequencing of 2709 regions across 69 lymphoma-related genes was performed on gDNA samples. Mutational calls were made in comparisons with individual control BM gDNA samples according to the criteria outlined in Table 1. All functional mutations detected in paired tumors per pt were compared, and shared and non-shared mutations were identified.
Results:
Baseline characteristics of the 19 pts were as follows: median age of 60 years (range, 32-77); 13 (68%) had stage I disease, and 11 (58%) had extranodal disease. At primary diagnosis, 14 of 19 pts (74%) had a non-germinal center B-cell-like (non-GCB) type DLBCL. As an initial treatment, CHOP therapy (median 4 cycles; range, 3-8), with (n=17) or without (n=2) radiation therapy, was performed in all 19 pts. Seven pts were treated with CHOP and rituximab.
The median duration from initial diagnosis to LR was 8 years (range, 5-18). At LR, the median age was 71 years (range, 45-84). One pt relapsed as a composite of DLBCL and indolent BCL, and two pts relapsed as indolent BCL.
Seven of the 19 pts were excluded from gene analysis because their paired gDNAs were of poor quality. The results of target sequencing combined with clinicopathological information and the results of IGH-PCR analysis are described in Table 2.
Shared mutations between individual pairs of primary and relapsed tumors were detected in nine of the 12 pts analyzed. The most frequent shared mutation was a CD79B missense mutation of a single base substitution in positions 196 (n=5) or 199 (n=2). The second most frequent mutation was a MYD88 (L265P) missense mutation (n=5). Co-mutation of CD79B and MYD88 was found in four pts, who were considered to have a MCD (MyD88,CD79b) type DLBCL (Schmitz et al. N Engl J Med 2018). All eight pts with a CD79B and/or MYD88 mutation had a non-GCB type DLBCL. The same clonal IGH rearrangements between paired tumors were found in six of the eight pts. Seven of the eight pts presented with primarily extranodal disease originating from the testis (n=3), nasal/paranasal cavity (n=2) or gingiva (n=2).
One pt (#9 in Table 2) with a GCB type DLBCL had shared mutations in MLL2, CREBBP, MEF2B and PIM1. However, different clonal IGH rearrangements were detected between paired tumors, implying these mutations may be the basis for lymphomagenesis; an on-going IGH rearrangement may occur.
In the other three pts (#10-12), shared mutations were not detected. Mutations in TP53 were not detected in any pts. We did not identify any specific mutations considered to be associated with LR.
Conclusions:
Common characteristics shared in a subgroup of pts with limited-stage DLBCL who developed LR were as follows: non-GCB type, CD79B and/or MYD88 mutations, and extranodal disease at primary manifestation. The mechanisms of LR from the viewpoint of gene alterations were considered heterogeneous.
Maruyama:Asahi Kasei Pharma: Honoraria; Takeda: Honoraria, Research Funding; Bristol-Myers Squibb: Honoraria; Dai-ichi-Sankyo: Honoraria; Dai-Nippon-Sumitomo: Honoraria; MSD: Honoraria, Research Funding; Chugai Pharma: Honoraria, Research Funding; Eisai: Honoraria, Research Funding; Fujifilm: Honoraria, Research Funding; Zenyaku Kogyo: Honoraria, Research Funding; AstraZeneca: Research Funding; Ono Pharmaceutical: Honoraria, Research Funding; Kyowa Hakko Kirin: Honoraria, Research Funding; GlaxoSmithKline: Research Funding; Abbvie: Research Funding; Astellas Pharma: Research Funding; Amgen Astellas BioPharma: Research Funding; Otsuka: Research Funding; Novartis: Research Funding; Nippon Boehringer Ingelheim: Research Funding; Pfizer: Research Funding; Solasia Pharma: Research Funding; Celgene: Honoraria, Research Funding; Biomedis International: Honoraria, Research Funding; Mundipharma International: Honoraria, Research Funding; Janssen: Honoraria, Research Funding. Izutsu:Amgen: Research Funding; Daiichi Sankyo: Honoraria, Research Funding; Kyowa Hakko Kirin: Honoraria; Bayer: Consultancy, Honoraria, Research Funding; Takeda: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding; MSD: Honoraria; HUYA Bioscience International: Research Funding; Celgene: Consultancy, Research Funding; Celltrion: Research Funding; Zenyaku: Research Funding; Sanofi: Research Funding; Gilead Sciences: Honoraria; Eisai: Honoraria, Research Funding; Novartis: Honoraria; Ono: Honoraria, Research Funding; Chugai: Honoraria, Research Funding; Nihon Medi-Physics: Honoraria; Symbio: Research Funding; Solasia: Research Funding; Mundhi: Honoraria; Otsuka: Honoraria; Bristol- Myers Squibb: Honoraria; Janssen: Honoraria, Research Funding; Astellas: Honoraria, Research Funding; Meiji Seika: Honoraria; Shionogi: Honoraria; Asahi Kasei: Honoraria. Tobinai:Takeda: Honoraria, Research Funding; SERVIER: Research Funding; Abbvie: Research Funding; Ono Pharmaceutical: Honoraria, Research Funding; Mundipharma: Honoraria, Research Funding; HUYA Bioscience International: Consultancy, Honoraria; Zenyaku Kogyo: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; GlaxoSmithKline: Research Funding; Chugai Pharma: Honoraria, Research Funding; Kyowa Hakko Kirin: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Eisai: Honoraria, Research Funding. Kobayashi:Pfizer: Research Funding; Ohtuka: Research Funding; Astellas: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal